The “angle” is the part of the eye where the iris meets the cornea and sclera. The drainage system of the eye is located at this region – trabecular meshwork .
Angle closure glaucoma typically affects anatomically “small eyes” – in which intra-ocular structures result in a crowded anterior segment. In primary angle closure glaucoma, the clogging of the angle by the peripheral iris will lead to IOP rise and damage to the optic nerve (see Angle closure glaucoma).
The contact between the iris and the trabecular meshwork represents a risk factor for the development of the disease. In these cases, regardless of normal IOP values and/or normal optic disc appearance, treatment may be indicated to prevent the sequence of events that may lead to angle closure glaucoma. Occludable angle diagnosis, with no other ocular abnormalities, means that the detection has been made early in the disease process.
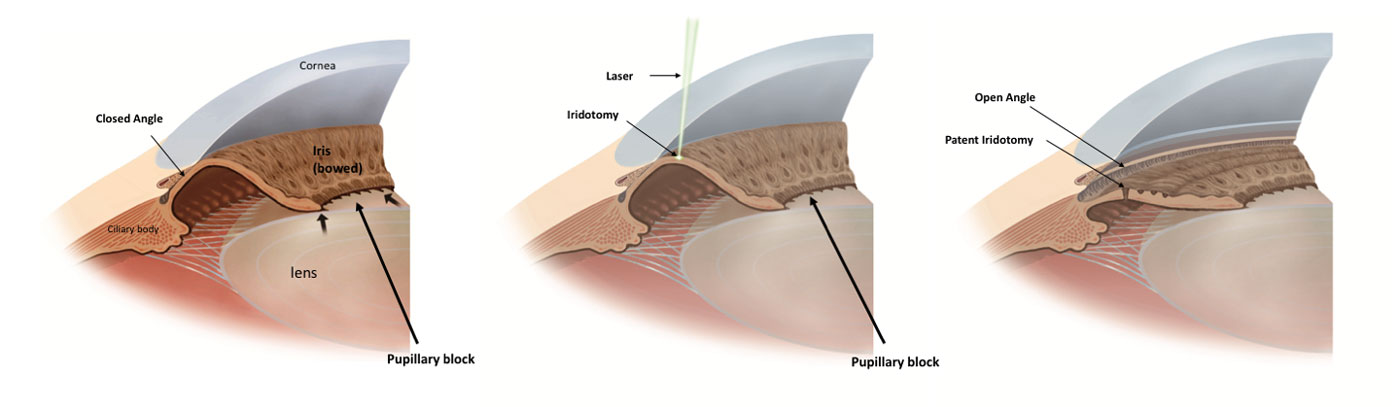
The most common mechanism of angle closure is called pupillary block, and it occurs due to relative block of fluid flow at the level of the pupil (from the posterior to anterior part of the eye), which causes forward bowing of the iris and narrowing of the angle (see Angle closure glaucoma).
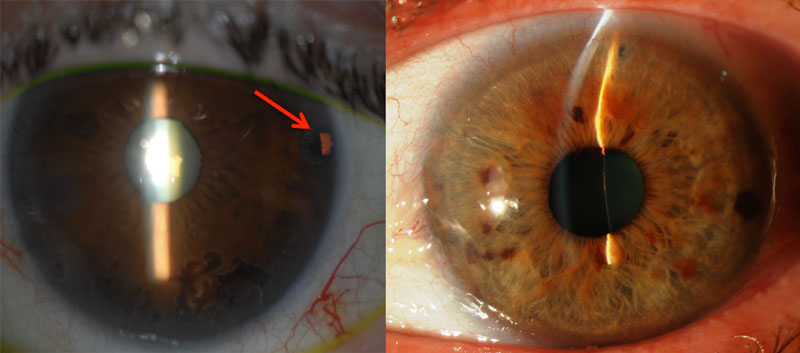
The usual therapy to be considered in the treatment of angle closure is laser iridotomy. This procedure will create a new communication between the anterior and posterior chamber (through the iris), and it aims to resolve pupillary block mechanism, resolving the forward bowing of the iris and, in most of the cases, open the angle (see Laser peripheral iridotomy). Cataract surgery, or removal of the natural lens and replacement with a thinner artificial lens, can also help opening the angle.